Measures of self-reported health status are generally considered fairly accurate measures of underlying “real” health status (measures of self-rated health (SRH) are, for example, predictive of subsequent mortality). Typical SRH items will ask a respondent something along the lines of “In general, how is the state of your health these days?” with a Likert response scale ranging between Very poor, Poor, Good and Very good, or a numbered item with up to 11 scale steps.
SRH is hugely successful in terms of cost-benefit ratios when compared to other ways of measuring individual level health, that would involve comparatively expensive and possibly intrusive medical procedures. In this regard, the measure is highly useful for researchers who need data on the health status of their respondents.
There is, however, an extremely important caveat to using this type of item: the measurement is only a valid predictor of health at a within-community level. That is, the measurement correlates with subsequent mortality only within groups of people who share a common frame of reference when it comes to what constitutes very poor or very good health. Intiutively, a respondent in Japan (which has the longest life expectancy in the world) who answers Good on an SRH item, will likely still be better off in terms of health than a respondent in Angola (which has among the shortest life expectancies in the world) who answers Very good. Subsequent mortality for the Japanese respondent is almost certainly going to be lower than for the Angolan respondent, despite the self-rated health being worse.
To see the consequences of this problem, consider as an example the following scatter diagram of average SRH reported in the World Values Surveys, and life expectancy, at the country level (data are for the latest year where both variables are measured).
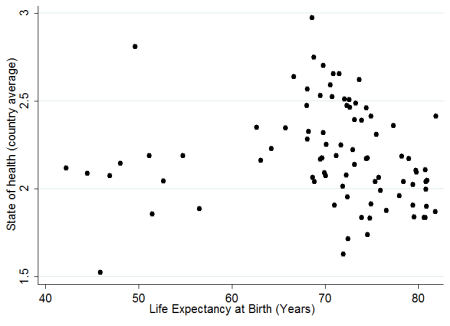
As we can see, there is basically zero correlation between self-rated health and life expectancy at the aggregate country level, which severely limits the practicability of using SRH in samples with individuals from (for example) different countries.
The lesson is that when using self-rated health measures in a study that contains individuals from different “health communities” (defined as units of individuals where perceptions of what constitutes a “normal” state of health are fairly consistent), it will be necessary to correct for this underlying heterogeneity of health perceptions. One possible way of doing this, if country-level variation is also utilized, could be to control for life expectancy (although it is quite likely that health perceptions will vary also within nations, for example between social classes). Another would be to simply dummy out between-group variation (or lack thereof) by classifying groups of people which plausibly belong to the same health communities, as defined above. Exactly how such units should best be defined remains an open empirical question, but a reasonable approximation could be dividing by nation and SES, and possibly gender.

